
One of the greatest challenges facing the NHS, in this its 70th anniversary year, is the care of ageing and increasingly frail older people. End of life care is not something that we as doctors seem to want to talk about, which means that when patients are admitted as an emergency to hospital the default is to treat them actively. This is most common if the patient is admitted at night by an out of hours doctor who doesn’t know them and is met by an on call junior doctor who doesn’t have the experience or the confidence to consider palliative care as a treatment option. Active treatment might well be and often is the correct course of action but in the absence of a discussion that has led to an advance care plan who is to know?
Against this background we have conducted a study of 10,477 patients admitted as medical emergencies to 22 Scottish hospitals during a two week period in March 2015 (1). The results are fascinating.
2,346 (22%) patients died in the year following the admission. One quarter of the deaths occurred during that admission and three quarters of the deaths occurred after discharge from hospital, commonly following readmission to hospital. Only 18% deaths occurred at home.
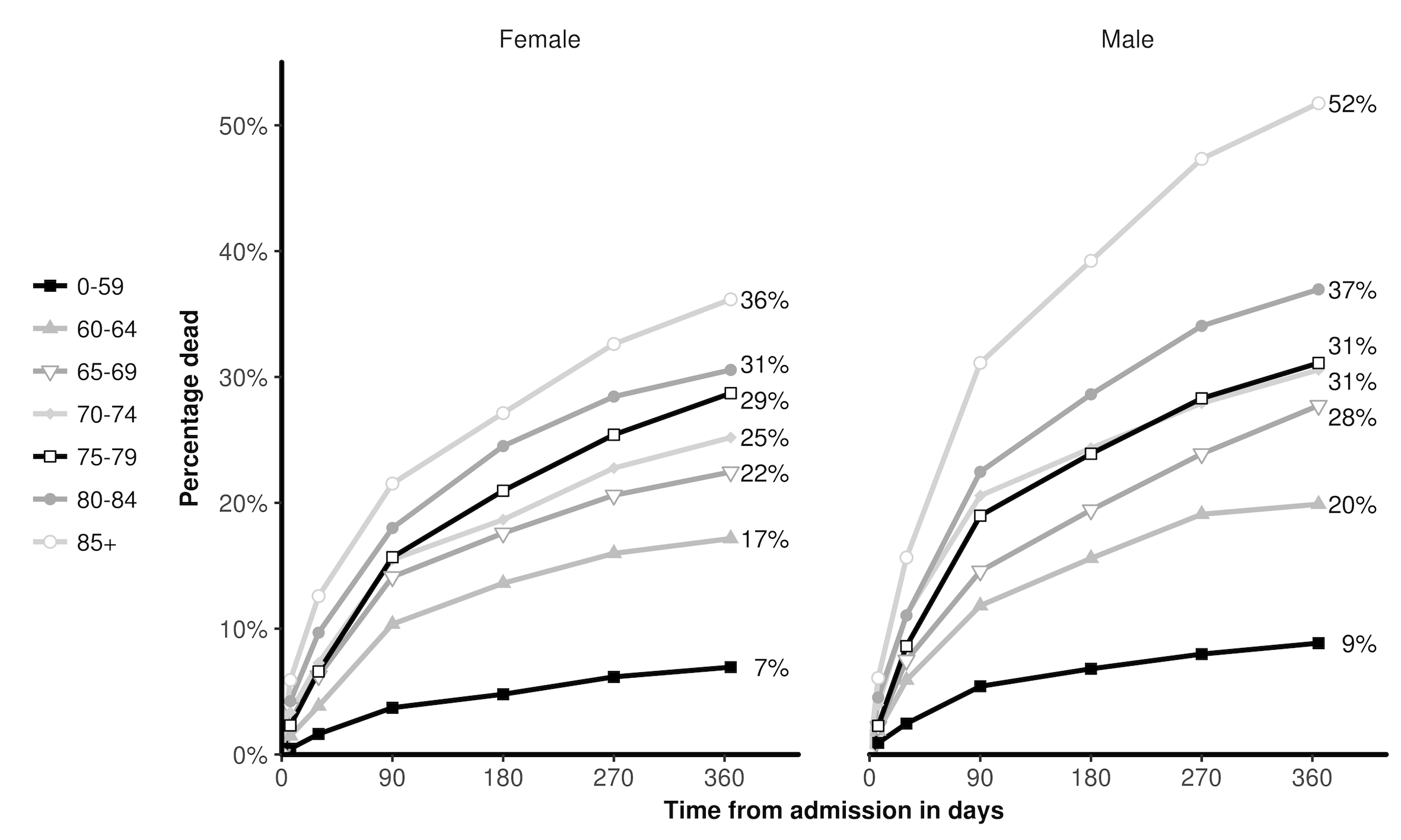
Cancers (34%), circulatory diseases (23%) and respiratory disease (18%) accounted for almost three quarters of all the deaths. Mortality rose steeply with age and was five times higher at one year for patients aged 85 years and over compared to those who were under 60 years of age (42% vs. 8%)
Cancer patients had a higher mortality rate than patients without a cancer diagnosis (56% vs. 17%). Mortality was also significantly higher among patients who had required one or more emergency admissions in the year before the census admission (30% vs 15%).
Another interesting feature of the study is the comparison of the likelihood of death in our group of emergency medical admissions with that of the Scottish population as a whole. The differences were striking. Our patient group was nine times more likely to die within a year than that of the comparable wider population.
These findings confirm and extend our previous work in Scotland (2) as well as studies in Ireland (3) and New Zealand (4). They indicate that it is possible to identify groups of patients admitted to hospital as medical emergencies who are at greatest risk of dying, not only during their hospital stay, but also in the following 12 months.
We believe these findings have important implications for health and social care and that they highlight a need for clinicians to alter their approach to patient care in order to identify and address key end of life care needs. This is a realistic, patient-focussed approach that has been widely advocated by the Gold Standards Framework (5), NICE (6), the General Medical Council (7), NHS England (8) and Health Improvement Scotland (9).
Here are some of the challenges:
- A National Confidential Enquiry into Patient Outcome and Death (NCEPOD) among patients who died within 30 days of receiving systemic anti-cancer therapy found that the decision to treat with chemotherapy was inappropriate in 19% cases. This raised questions as to whether cancer patients are given enough information about chemotherapy to enable them to make an informed consent to treatment (10).
- In a study of patients with metastatic lung and colorectal cancer, 69% and 81% of patients respectively were unaware that chemotherapy was highly unlikely to cure their cancer, again suggesting that clinicians are not comfortable with end of life care discussions (11).
- A survey of over 4000 American physicians found that one third would not discuss prognosis with a cancer patient who was asymptomatic but had only 4-6 months to live, preferring instead to wait until symptoms developed or there were no more treatments to offer (12).
- Up to 26% cancer patients, 59% of those with organ failure and 34% with frailty do not have advance care plans in place before death (13). Too often the discussion with patient and family is avoided.
We believe that our findings support the view that emergency admission to hospital provides an important opportunity to have conversations and to make advance care plans, if appropriate, relating to end of life care. We believe all clinicians involved in caring for patients at or near the end of life have a responsibility to communicate effectively with patients, their families and members of the multi-disciplinary team in order to explore treatment goals and make key decisions.
Good advance care planning in hospital could mean that the next time a frail older patient becomes unwell, a course of action ensues which does not result in emergency admission to hospital.
Professor Chris Isles is a consultant physician currently working in acute medicine at Dumfries and Galloway Royal Infirmary in south west Scotland. He has a long standing clinical interest in end of life care, has published extensively in the fields of hypertension, cardiology and renal disease, and has collaborated with Professor Clark at the University of Glasgow on two previous end of life papers.
References
- Moore E, Munoz-Arroyo R, Schofield L et al. Death within one year among emergency medical admissions to Scottish hospitals: incident cohort study. BMJ Open 2018; 8: e0214342. Doi:10.1136/bmjopen-2017-021432
- Clark D, Armstrong M, Allan A, Graham F, Carnon A, Isles C.. Imminence of death among hospital inpatients: prevalent cohort study. Palliative Medicine 2014; 28: 474-479.
- Kellett J, Rasool S, McLoughlin B. Prediction of mortality 1 year after hospital admission. Q J Med 2012; 105:847-853
- Gott M, Broad J, Zhang X, Jarlbaek L, Clark D. Likelihood of death among hospital inpatients in New Zealand: prevalent cohort study. BMJ Open 2017; 7: e016880. Doi:10.1136/bmjopen-2-17-016880
- The Gold Standards Framework Proactive Identification Guidance, 2016. Accessed at www.goldstandardsframework.org.uk/PIG 10th September 2017
- NICE Quality Standard 13. End of life care for adults. First published 28th November 2011. Accessed at www.nice.org.uk/guidance/qs13, 10th September 2017
- General Medical Council. Treatment and care towards the end of life: good practice in decision making. First published 20th May 2010. Accessed at www.gmc-uk.org/guidance/ethical_guidance/end_of_life_care 10th September 2017
- NHS England. Actions for end of life care: 2014-2016. First published 11th November 2014. Accessed at www.england.nhs.uk/actions-eolc on 10th September 2017
- Health Improvement Scotland. Palliative and end of life care. First published March 2013. Accessed at www.healthcareimprovementscotland.org on 10th September 2017
- Mort D, Lansdown M, Smith N, Protopapa K, Mason M. For better or worse? A report by the National Confidential Enquiry into Patient Outcome and Death, 2008. Accessed at https://www.ncepod.org.uk/SACT-report on 4th October 2017
- Weeks JC, Catalans PJ, Cronin A et al. Patients’ expectations about effects of chemotherapy for advanced cancer. N Engl J Med 2012; 367: 1616-25
- Keating NL, Landrum MB, Rogers SO et al. Physician factors associated with discussions about end of life care. Cancer 2010; 116: 998-1006
- Tapsfield J, Hall C, Lunan C, McCutcheon H, McLoughlin P, Rhee J et al. Many people in Scotland now benefit from anticipatory Care before they die: an after death analysis and interviews with general practitioners. BMJ Supportive and Palliative Care 2016. Accessed online doi:10.1136/bmjspcare-2015-001014